Lambing Emergencies: A Field Guide and Series Overview
A hypothermic lamb older than five hours that you warm without first giving glucose will seize and die. A retained placenta that you pull tears the caruncular attachments and causes severe hemorrhage. A ewe with milk fever and a ewe with pregnancy toxemia look identical in the field, and the wrong-only treatment for either kills her on a slower clock.
This is the kind of detail we wish we had memorized before our first lambing season. We did not. We are not veterinarians, we are not extension agents, and we are not experienced shepherds. This is our first season with Katahdin sheep, and the six-part series this article overviews was written first for ourselves - a working reference we built from primary sources during the months before lambing started, so we would not have to think clearly under stress about things we could decide ahead of time.
We did not run into every complication on this list - far from it. But it became clear very quickly, often in the first week of lambs on the ground, how unprepared and inexperienced we actually were. The kit was incomplete in places we had not anticipated. The protocols we thought we had memorized turned out to be the ones we had only skimmed. The ewe behaviors we had read about looked different in person than they did in extension photos. We learned by being caught short, asking the vet, and writing down what we should have known. This article is the version of that working reference we wish someone had handed us in February.
We put it online because the same gaps that nearly caught us out probably catch out other first-season shepherds, and the information is free to share. It is not a substitute for a relationship with a livestock veterinarian, a mentor, or your local extension office. It assists, it does not replace. If you are reading this in an actual emergency, call your vet first, then come back to the protocols.
Why This Article Exists Alongside the Series
The six-part series covers the structural arc of a lambing season: preparation, the labor itself, rejection and bottle lambs, first-weeks procedures, first-year health, and yearling growth and selection. It is long, and it is organized by chronology rather than by emergency.
This article inverts that. It is the quick-reference layer on top of the series, focused on the six complication categories that actually kill lambs and ewes in the first 72 hours. The 5-hour rule is the centerpiece because it is the single piece of information most likely to flip an outcome the wrong way if a well-meaning shepherd applies the obvious-but-wrong protocol.
The series:
- Part 1: Preparation and Supplies - what to have staged in the barn before day 140 of gestation
- Part 2: Field Observations During Labor - the labor itself and the first 72 hours
- Part 3: Rejection Protocols - rejection, grafting, and the bottle-lamb decision
- Part 4: First-Weeks Procedures - tagging, castration, scrapie, pain management
- Part 5: First-Year Health - vaccines, FAMACHA, parasites, coccidiosis
- Part 6: NSIP, Growth, and Selection - measurement-driven selection through the yearling
If you read nothing else from this site before your first lambing, read Part 1 (so the kit is in the barn) and the rest of this article (so you know what to do with the kit when something goes wrong).
Pregnancy Toxemia: The Metabolic Emergency You Prevent
Pregnancy toxemia, also called twin-lamb disease or ketosis, is the most important metabolic emergency in late-gestation ewes, and almost all of it is preventable. The condition develops when energy demand from multiple fetuses outstrips the ewe's glucose supply, and the cascade runs through three stages with progressively worse prognosis.
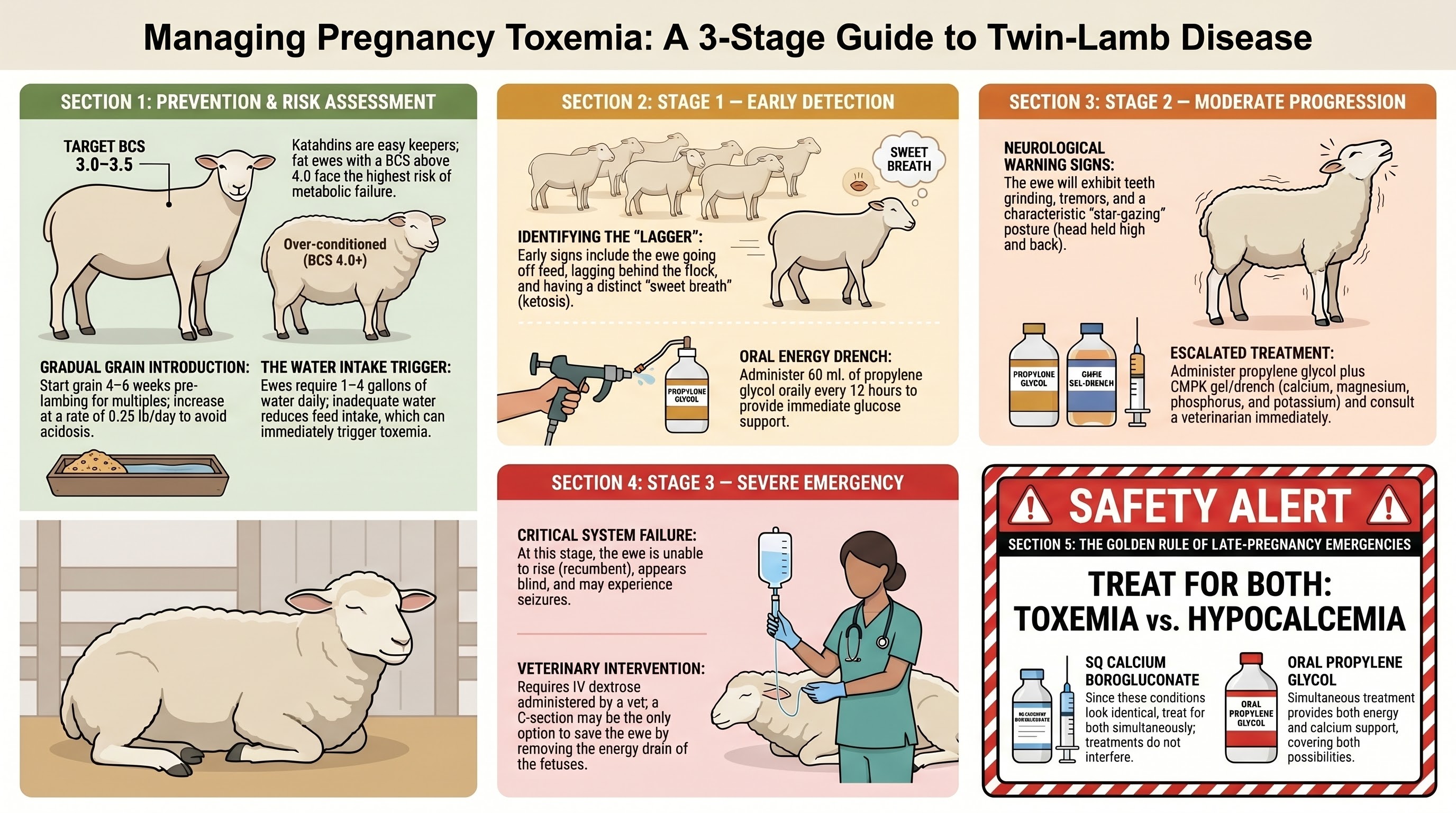
The critical prevention insight is counterintuitive: fat ewes are at highest risk, not thin ones. A body condition score above 4.0 going into late gestation is a red flag. The liver becomes infiltrated with fat to the point where it cannot handle the metabolic demand of the final six weeks. Maintaining BCS 3.0 to 3.5 at lambing, with a gradual grain introduction starting six weeks before lambing, prevents the condition in the vast majority of small flocks.
Field treatment by stage:
| Stage | Signs | Treatment |
|---|---|---|
| Early | Lagging behind flock, off feed, sweet/fruity breath | 60 mL propylene glycol orally every 12 hours |
| Moderate | Teeth grinding, "star-gazing" posture, tremors | Propylene glycol plus CMPK plus vet consult |
| Severe | Unable to rise, apparent blindness, seizures | IV dextrose by vet; C-section may be required |
UK guidance from veterinary references adds a field option: 50 to 100 mL of 40 percent glucose subcutaneously plus 50 mL propylene glycol orally where IV dextrose is not immediately available. The Merck Veterinary Manual is the canonical reference for the staged protocol.
The 5-Hour Hypothermia Rule
This is the rule that should be tattooed on the inside of every lambing-barn door.
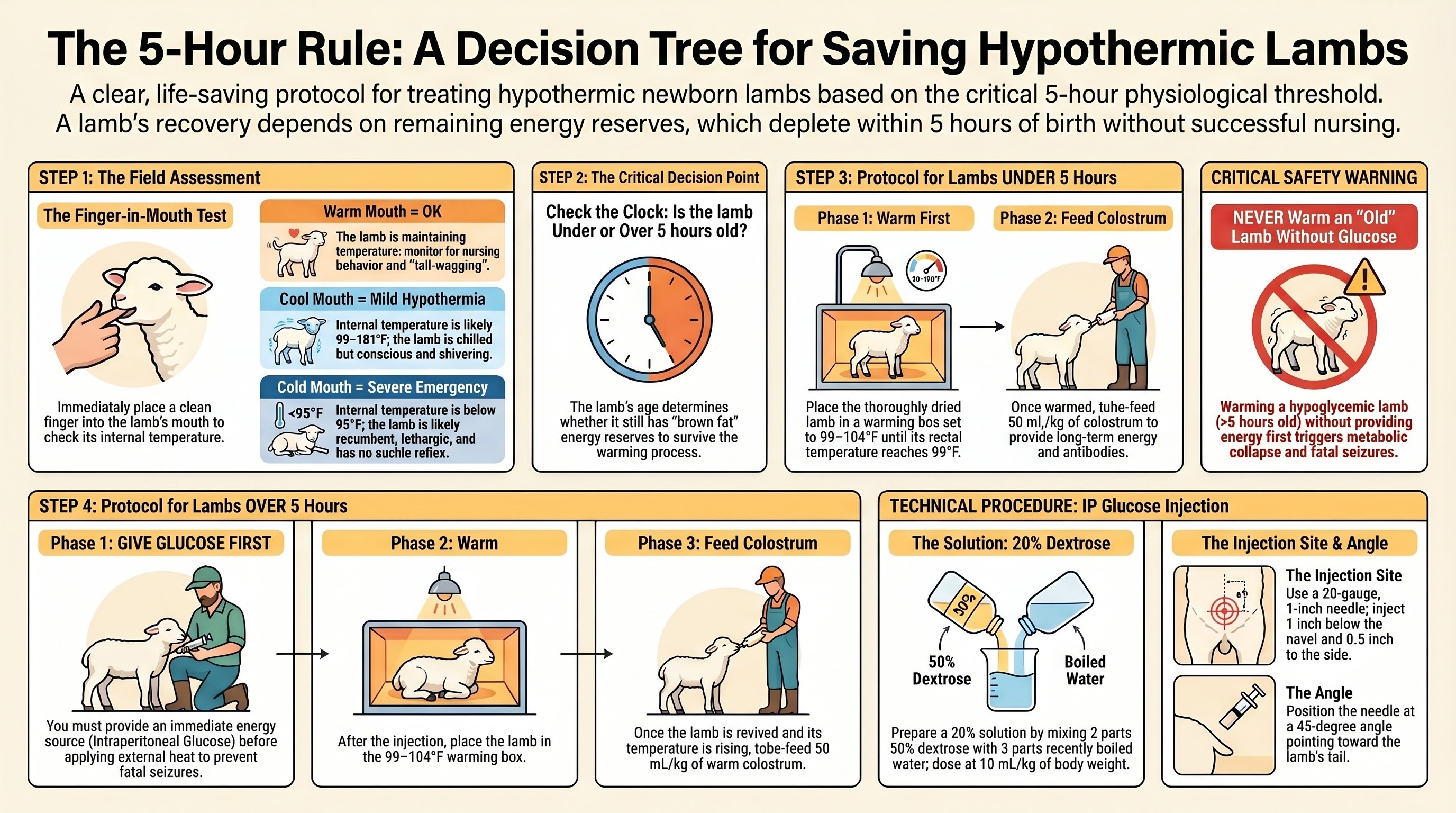
Newborn lambs are born with brown adipose tissue - specialized fat that generates heat through non-shivering thermogenesis. In the first five hours after birth, that brown fat is the lamb's energy reserve. Beyond about five hours, the brown fat is depleted, and a lamb that is hypothermic at that point is also, almost certainly, hypoglycemic.
The decision branches:
- Lamb under 5 hours old, hypothermic. Dry thoroughly. Warm in a warming box to 99°F. Tube colostrum once warm. Brown fat reserves carry the lamb through the warming period.
- Lamb over 5 hours old, hypothermic. Give intraperitoneal glucose first - 10 mL/kg of 20 percent dextrose, injected one inch below the navel at a 45-degree angle pointed toward the tail. Then warm. Then tube colostrum.
Warming a hypoglycemic lamb without correcting the glucose first triggers fatal seizures as the brain attempts to resume function without available glucose. This is the single piece of information most likely to be applied backwards by a shepherd doing the intuitive thing.
The field check is simple: slip a finger into the lamb's mouth.
- Warm mouth - core temperature adequate, simple monitoring sufficient
- Cool mouth - mild hypothermia, warm and tube
- Cold mouth - severe emergency, IP glucose first if over five hours
Mark every lamb's birth time on its body with a livestock marker. The 5-hour rule cannot be applied without knowing the lamb's age. We did not do this on our first few lambs and had to estimate from the dam's labor timeline, which is exactly the kind of avoidable cognitive load you do not need at 2 a.m.
NADIS, the Merck Veterinary Manual, Penn State Extension, and NIH-indexed neonatal lamb-care literature converge on this protocol. It is not contested.
Six Malpresentations and How to Correct Them
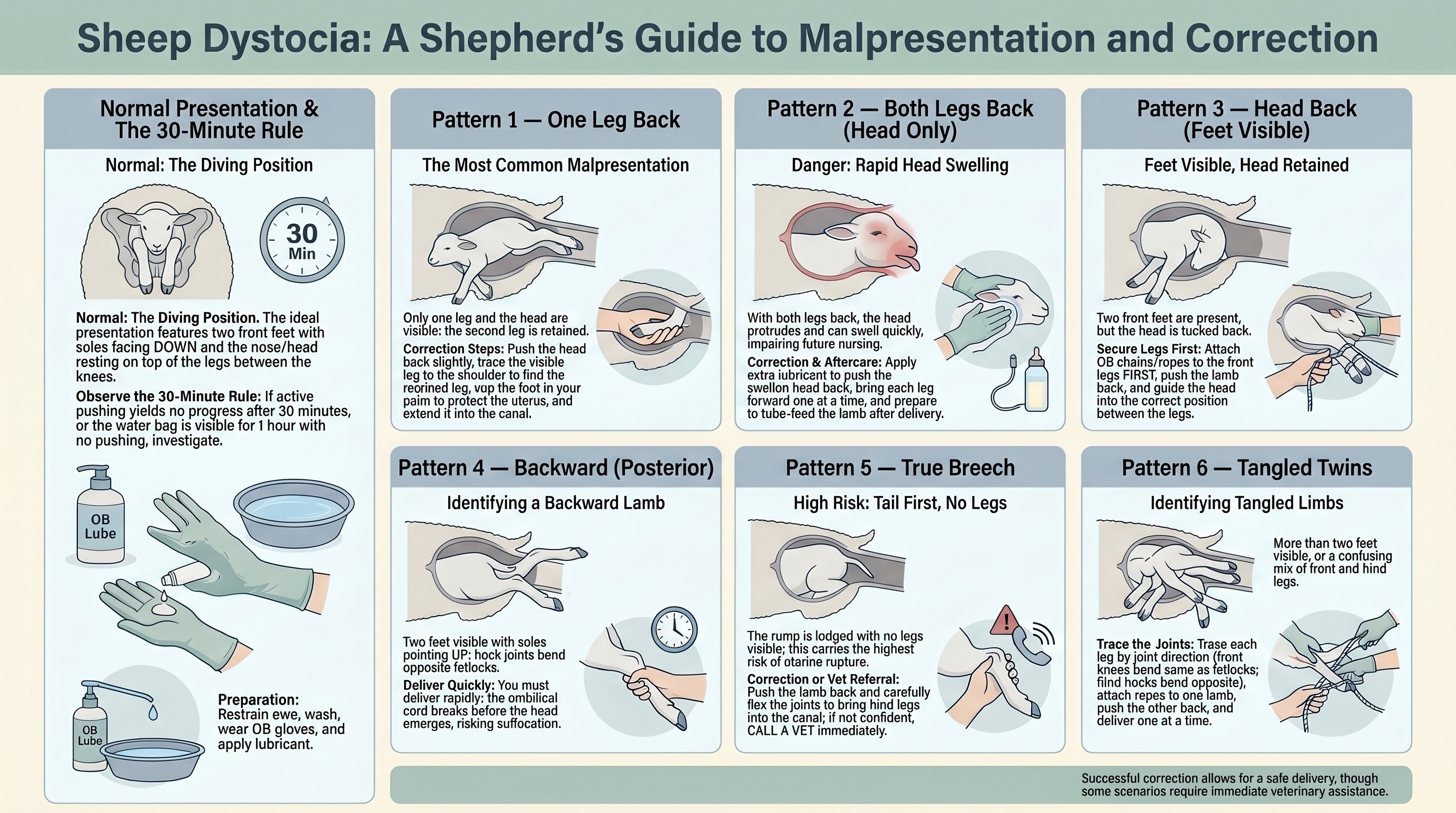
Normal presentation is two front feet and nose visible at the vulva - the "diving position." Anything else is a malpresentation, and each pattern has a specific correction sequence. Skill at correcting malpresentations is what separates a shepherd from someone who calls the vet for every difficult delivery, but knowing your own limits is what separates a shepherd from someone who tears a uterus.
Brief reference table:
| Pattern | Visible signs | Correction |
|---|---|---|
| One leg back | Most common; one front foot and nose | Push head back, trace free leg to shoulder, cup foot in palm, extend into canal |
| Both legs back | Head protruding, no legs | Push swollen head back with lubricant, bring each leg forward; tube feed lamb after (swollen tongue impairs nursing) |
| Head back | Two front feet, no head | Attach OB chains to front legs FIRST so you do not lose them, push lamb back, guide head between legs |
| Backward (posterior) | Soles facing up | Deliver QUICKLY - umbilical cord breaks before the head emerges, lamb has seconds to minutes |
| True breech | Tail first, no legs visible | Highest uterine rupture risk - call vet if not confident |
| Twins tangled | Multiple legs, unclear which belong to which lamb | Trace each leg by joint direction, attach ropes, deliver one at a time |
Backward (posterior) presentation is worth special emphasis: because the umbilical cord breaks against the pelvic brim before the head clears the canal, asphyxia risk is high. Once you confirm a posterior, deliver fast. This is not a presentation where you take time to prepare - the lamb is on a clock that started the moment the cord broke.
The Merck Veterinary Manual, NADIS, and Ohio State Extension publish photo references for each pattern. Spend an evening before lambing season studying those references. A correction you have rehearsed mentally is faster than a correction you are working out in real time with one arm inside the ewe.
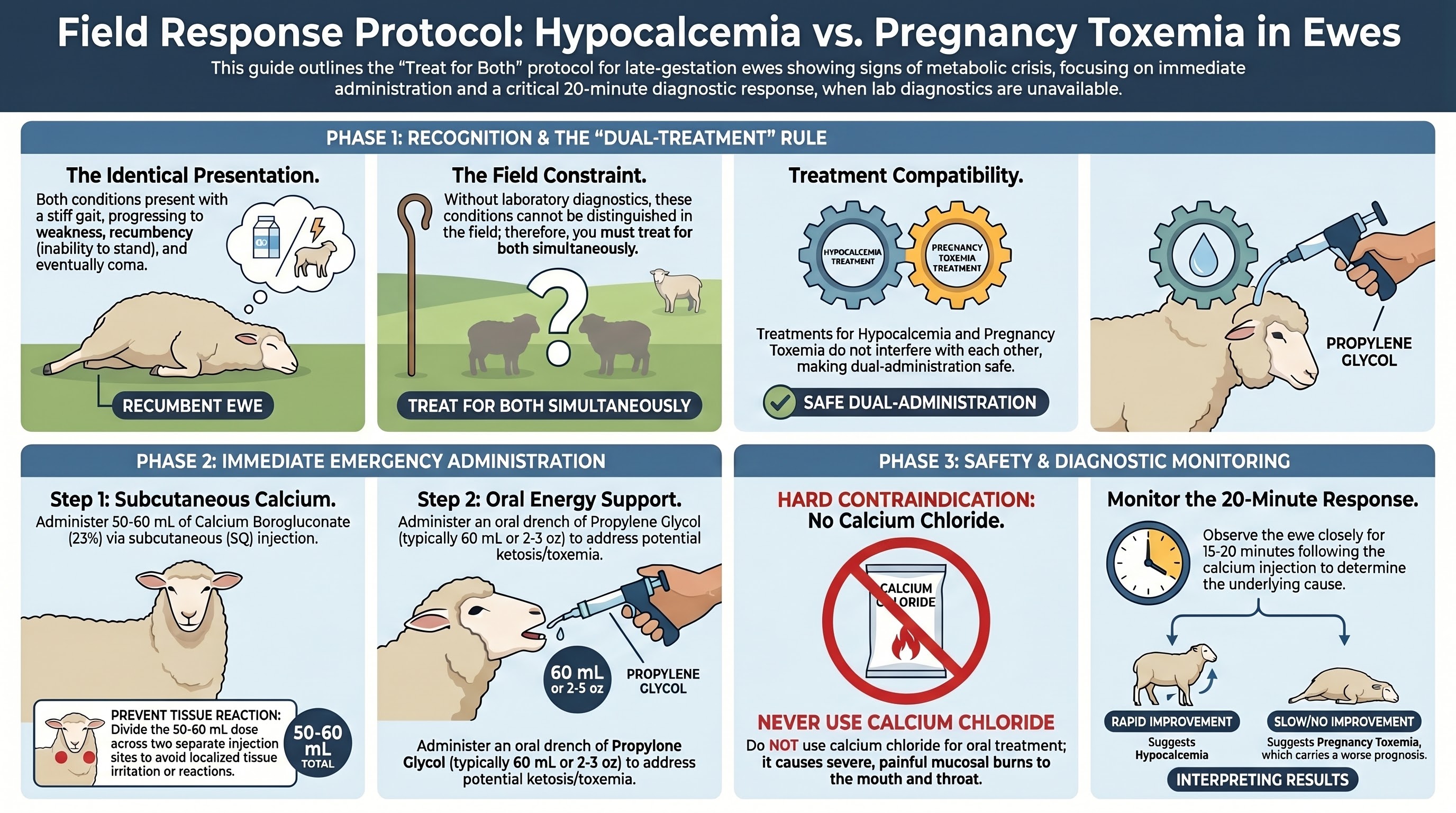
When the Differential Is Impossible: Treat Both
Hypocalcemia (milk fever in sheep) and pregnancy toxemia present with nearly identical clinical signs - stiff gait, progressive weakness, recumbency, eventually coma. Without lab diagnostics, you cannot reliably distinguish them in the field. The literature is unusually direct about the practical resolution.
The protocol:
- Calcium borogluconate 23 percent, 50 to 60 mL subcutaneous, divided across two injection sites to avoid tissue reaction
- Plus propylene glycol orally, same dosing as the toxemia protocol
The treatments do not interfere with each other. Rapid improvement within 15 to 20 minutes after the calcium injection points strongly to hypocalcemia. Slow or absent improvement points to toxemia, which has a worse prognosis and may require vet escalation.
One firm contraindication: do not use calcium chloride for this treatment. Unlike calcium borogluconate, it causes severe mucosal burns to the mouth and throat. The two compounds sound similar; they are not interchangeable.
For neonatal lambs in the 12-to-72-hour range, watery mouth disease (E. coli enterotoxemia, often associated with insufficient or delayed colostrum) is treated with oral electrolytes at 50 mL/kg four times daily. Soapy-water enemas can promote gut activity. The differential here is clinical: depressed lamb, drooling, often with insufficient colostrum history.
Two Post-Delivery Emergencies, Opposite Interventions
Uterine prolapse and retained placenta both occur in the hours after delivery and both can be fatal. The interventions are exact opposites.
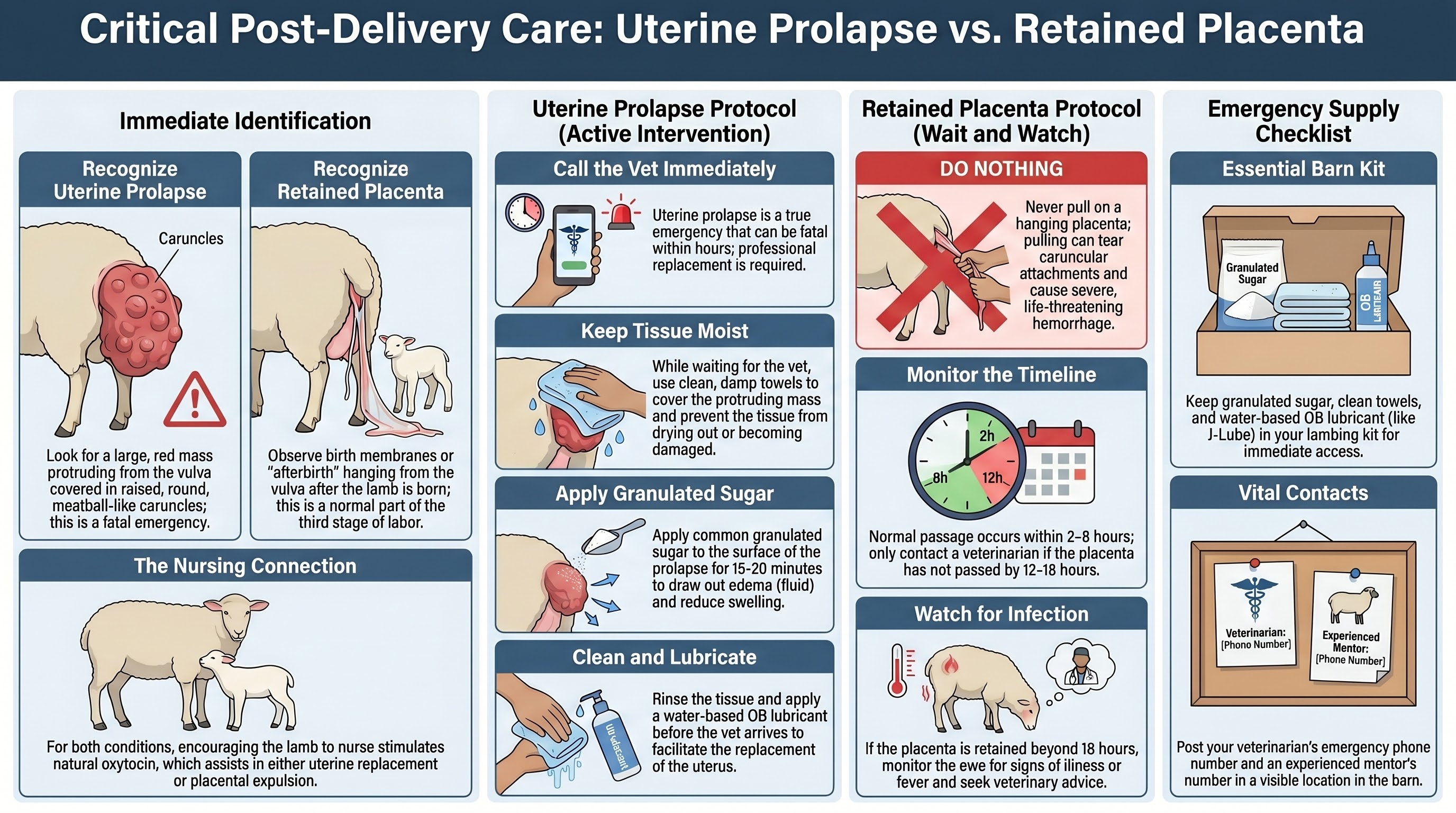
Uterine prolapse - large tissue mass with rounded raised caruncles protruding from the vulva - is a true emergency, fatal within hours if not properly replaced. Call the vet immediately. While waiting:
- Keep the tissue moist with damp towels
- Apply granulated sugar to the surface to draw edema fluid and reduce swelling (rinse and lubricate before the vet attempts replacement)
- Encourage the lamb to nurse - oxytocin from nursing may assist with replacement
Unlike vaginal prolapse, uterine prolapse has no documented genetic component, so the ewe does not necessarily get culled if she recovers cleanly.
Retained placenta is the opposite case: do nothing. Pulling tears the caruncular attachments and causes severe hemorrhage. Normal placental passage is two to eight hours after delivery. Call the placenta retained if it has not passed by 12 to 18 hours. Monitor for infection. Contact the vet if the ewe shows systemic illness. Continued nursing by the lamb stimulates oxytocin release that aids natural expulsion.
The reflex to "help" the ewe is exactly wrong here. Patience and observation are the intervention.
Post-Dystocia Rejection: The First-Hour Decision
The final emergency category is the one most often mismanaged through optimism. A ewe who required intervention to deliver - pulled lamb, malpresentation correction, C-section - is at sharply elevated risk of rejecting her offspring. The mechanism is neurological: normal maternal bonding depends on an oxytocin surge triggered by birth-canal stimulation, and assisted delivery interrupts that stimulation. Pain and stress further suppress the response.
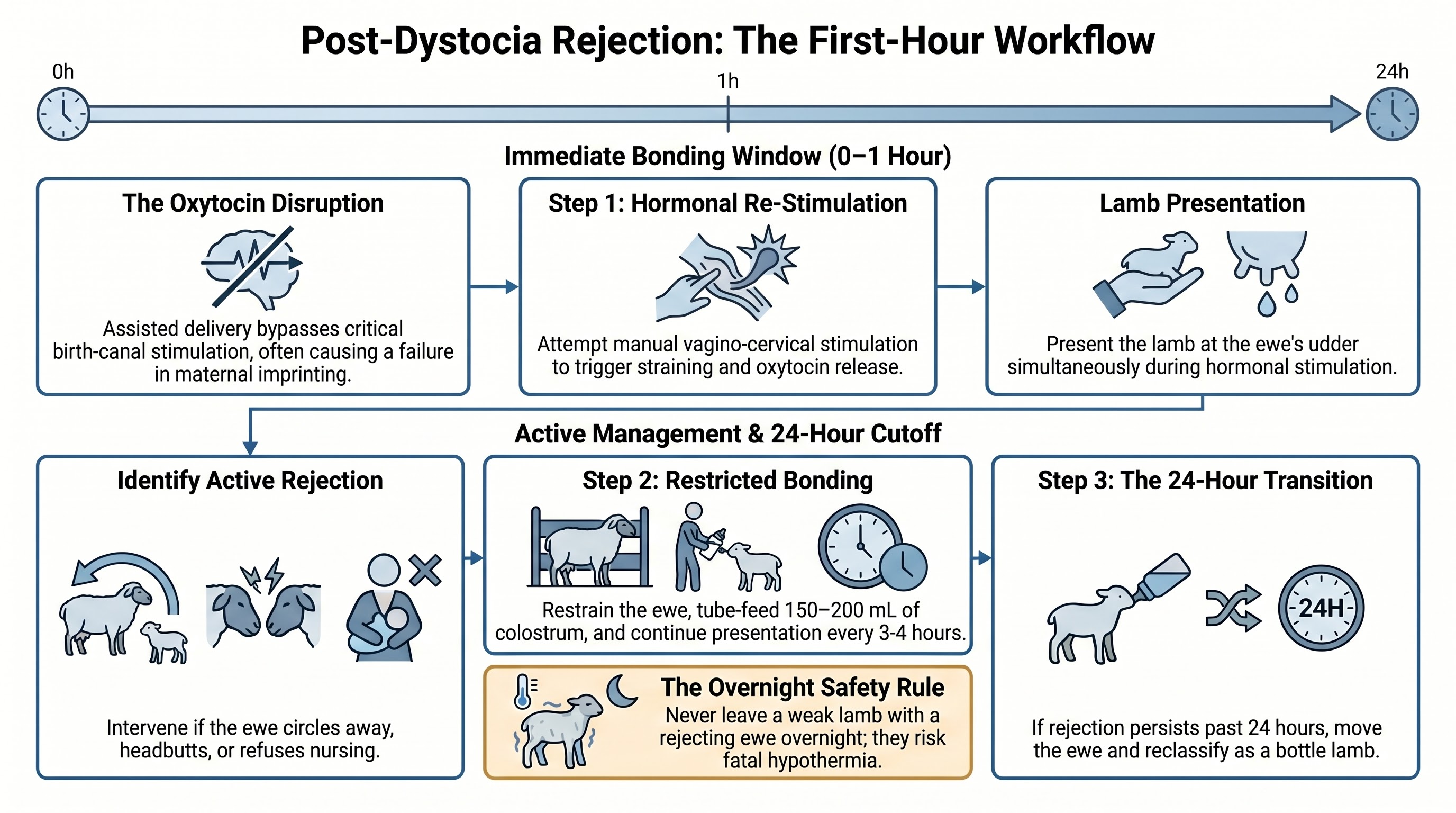
The response window is the first hour. In priority order:
- Vagino-cervical stimulation of the ewe - manual stimulation of the birth canal to reopen the hormonal bonding window - while presenting the lamb at the udder.
- If active rejection persists (headbutting, circling, refusing to allow nursing), confine the ewe in a lambing jug with restraint and tube-feed the lamb 150 to 200 mL of colostrum from her by hand while continuing presentation attempts.
- If rejection persists past 24 hours, reclassify the lamb as a bottle lamb and move it to the bottle protocol described in Part 3.
The failure mode to avoid: leaving a weak post-dystocia lamb with a rejecting ewe overnight in the hope that bonding will settle on its own. By morning, the lamb will be hypothermic and hypoglycemic. NIH-indexed research on neonatal lamb mortality identifies failed early recognition of rejection as a leading cause of preventable lamb loss.
The Lambing Kit, Staged Before Day 140
These six emergencies are not independent - they cluster. A ewe who experienced pregnancy toxemia may have a weakened delivery, leading to a malpresentation, leading to a pulled lamb, leading to rejection, leading to lamb hypothermia and hypoglycemia. The shepherd who has prepared for one of them and not the others gets caught by the cascade.
The kit, staged in the barn before the first due date:
- Propylene glycol (toxemia stages 1 and 2)
- Calcium borogluconate 23 percent and 18-gauge needles (hypocalcemia)
- 20 percent dextrose, 60 cc syringes, 18-gauge needles (5-hour-rule IP glucose)
- OB chains and obstetric lubricant (malpresentations)
- Warming box with thermometer (hypothermia)
- Granulated sugar (uterine prolapse, while waiting for vet)
- Lamb feeding tube and 60 cc syringe (tube colostrum)
- Livestock marker (mark every lamb's birth time)
- Vet phone number, posted in the barn at eye level
Part 1 of the series covers the broader supply list and the calendar that drives when each item must be operational. The list above is the strict subset that is in play during an actual emergency.
A Pause Point, Not a Conclusion
We are first-season shepherds writing to other people who might be in the same position. Everything above came from veterinary references and extension publications, not from our own clinical experience, because we do not have clinical experience yet. We had a vet on speed-dial through our first lambing and we used the relationship - and we are still going to use it. The protocols above shorten the time between recognizing a problem and starting the right intervention; they do not replace professional judgment about when an animal needs more than a kit can provide.
If you are using this article, build a relationship with a livestock veterinarian before lambing season starts. Most rural vets will do a pre-lambing barn visit for a flat fee. Use it. Ask which emergencies you should attempt yourself and which you should hand off. Ask whether the dosing in the references applies to the body weights of your specific ewes. The answers vary by region, by veterinarian, and by ewe. The protocols above are a starting point for that conversation, not the conversation itself.
We hope this is useful. We also hope you do not need it.
Series navigation: Part 1: Preparation and Supplies - Part 2: Field Observations - Part 3: Rejection Protocols - Part 4: First-Weeks Procedures - Part 5: First-Year Health - Part 6: NSIP, Growth, and Selection
This article synthesizes research from the Merck Veterinary Manual, NADIS (National Animal Disease Information Service), Penn State Extension, Ohio State University Extension, NIH-indexed peer-reviewed studies on neonatal lamb mortality, Craig Robinson Vets, and Capontree Vets. It is a practical reference written by first-season shepherds for first-season shepherds, and it is not a substitute for veterinary advice. Always consult your veterinarian for medical decisions specific to your flock.